Metastases to the breast from extramammary malignancies
To:
To:
p. 470
Tanvi Vaidya, Subhash Ramani, Ashita Rastogi
DOI:10.4103/ijri.IJRI_218_18
Metastases to the breast from extra-mammary malignancies are extremely uncommon. The discovery of a breast mass in a patient with a known primary tumor elsewhere poses a diagnostic challenge to the clinician. An awareness of the various malignancies that can metastasize to the breast and accurate diagnosis of the same is essential to avoid an unnecessary mastectomy and to guide further therapy. In this case series, we describe such clinical scenarios with an emphasis on the imaging features of metastases to the breast, which will enable radiologists to recognize this entity with greater ease.
http://www.ijri.org/currentissue.asp?sabs=y






Tanvi Vaidya, Subhash Ramani, Ashita Rastogi
DOI:10.4103/ijri.IJRI_218_18
Metastases to the breast from extra-mammary malignancies are extremely uncommon. The discovery of a breast mass in a patient with a known primary tumor elsewhere poses a diagnostic challenge to the clinician. An awareness of the various malignancies that can metastasize to the breast and accurate diagnosis of the same is essential to avoid an unnecessary mastectomy and to guide further therapy. In this case series, we describe such clinical scenarios with an emphasis on the imaging features of metastases to the breast, which will enable radiologists to recognize this entity with greater ease.
http://www.ijri.org/currentissue.asp?sabs=y

Metastases to the breast from extra-mammary malignancies are extremely uncommon, with a prevalence ranging from 1.7% to 6.6%.[1] The most common sources of metastases to the breast are lymphomas/leukemias and melanomas. Rare primary tumors to metastasize to the breast include carcinomas of the lung, ovary, and stomach, and even more uncommonly carcinoid tumors, hypernephromas, carcinomas of the liver, tonsil, pleura, pancreas, cervix, endometrium, and bladder. The dissemination occurs via both hematogenous and lymphatic routes.[1],[2]
The discovery of a breast mass in a patient with a known primary tumor elsewhere or with a previous history of cancer at another site poses a diagnostic challenge to the clinician. An awareness of the various malignancies that can metastasize to the breast and accurate diagnosis of the same is essential in order to avoid an unnecessary mastectomy and to guide further therapy.
In this article, we present six cases of metastases to the breast, in patients with a primary extramammary malignancy. Metastases in these primary tumors are exceedingly rare, and hence, this case series would serve as a valuable addition to the existing literature. In addition, we present a review on the subject with an emphasis on imaging findings.
Case 1
A 40-year-old lady presented with menorrhagia for about 8 months. She underwent a contrast-enhanced CT scan of the abdomen and pelvis, which revealed a heterogeneously enhancing myometrial mass, with atypical imaging features [Figure 1]A. There was no evidence of distant metastases on cross-sectional imaging. The patient underwent a total hysterectomy with a bilateral salpingo-oophorectomy. Histopathological evaluation of the myometrial mass revealed an intermediate grade leiomyosarcoma (Immunohistochemistry IHC – Mib labeling index of 50%). Thereafter, she presented with a lump in the right breast, progressively increasing in size over a period of 6 months.
Mammography revealed the presence of a well-circumscribed isodense mass in the upper outer quadrant of the right breast [Figure 1]C and [Figure 1]D. Breast ultrasonography demonstrated a well-defined solid, hypoechoic mass with mild posterior acoustic enhancement, at the site of palpable abnormality [Figure 1]B. A core biopsy of the lesion revealed a spindle cell tumor exhibiting focally moderate to marked nuclear atypia. On IHC, tumor cells were positive for smooth muscle actin, desmin, H-caldesmon and showed a high Mib-1 count. The histopathology report was conclusive for leiomyosarcoma in the clinical context. A contrast-enhanced CT abdomen scan was subsequently done which revealed a metastatic lesion in the liver and a retroperitoneal metastatic nodal mass. Thereafter, the patient received palliative chemotherapy for 2 years but did not survive.
Case 2
A 31-year-old lady, with poorly differentiated adenocarcinoma of the stomach (stage T3N2M0), underwent a radical gastrectomy. She was receiving adjuvant chemo-radiotherapy (CT-RT) during which she developed abdominal distention, along with diffuse pain in the left breast with redness of the overlying skin over a period of 1 month. A contrast-enhanced CT scan of the thorax and abdomen with a mammogram was performed. Contrast-enhanced CT of the thorax and abdomen revealed ill-defined enhancement in the left breast [Figure 2]A.
Mammography revealed a diffuse increase in density involving the left breast, with thickening of the overlying skin and the nipple–areola complex [Figure 2]B. Breast ultrasonography demonstrated an ill-defined hypoechoic lesion replacing the fibro-glandular parenchyma [Figure 2]C. A left breast core biopsy revealed poorly differentiated carcinoma with signet ring cell morphology. Immunohistochemistry revealed positivity for CK 7, ER, CDX2, CK 20, and GCDFP, which was consistent with metastasis from carcinoma stomach. Contrast-enhanced CT abdomen revealed ascites with peritoneal metastases. The patient is being treated with palliative chemotherapy since then, with stable disease.
Case 3
A 37-year-old lady, with carcinoma cervix (stage IIIa) receiving concomitant chemoradiation and brachytherapy for the same, developed a lump in the left breast, gradually increasing over a period of 3 months. A mammogram and a screening ultrasonography of the abdomen were performed.
Mammography revealed a well-circumscribed, isodense mass in the upper central region of the left breast [Figure 3]A and [Figure 3]B. A breast ultrasound revealed a predominantly hypoechoic lesion in the upper central region showing mild internal vascularity [Figure 3]C. Fine-needle aspiration of the lesion revealed clusters of squamous epithelial cells, consistent with metastasis from cervical carcinoma. An ultrasound of the abdomen revealed evidence of liver metastases. The patient was put on palliative chemotherapy, is now being followed up annually.
Case 4
A 16-year-old girl, with Ewing's sarcoma of the left ninth rib being treated with chemotherapy, presented with a slow growing lump in the left breast. About 3 months after commencement of therapy, a contrast-enhanced CT of the thorax was performed for monitoring disease response. The CT revealed a heterogeneously enhancing mass involving the left ninth rib causing bony destruction with intrathoracic extension. In addition, an irregular heterogeneously enhancing mass with central necrosis was also seen incidentally in the left breast. Bilateral pleural effusion was seen [Figure 4]A,[Figure 4]B,[Figure 4]C. A breast ultrasound revealed a predominantly hypoechoic mass with irregular margins in the upper central region [Figure 4]D. A fine-needle aspiration cytology study of the left breast mass revealed cytologic features of PNET (Primitive neuro-ectodermal tumor)/Ewing's sarcoma with positivity for CD99, consistent with metastases from the primary. The patient was treated with systemic chemotherapy and received radiotherapy to the breast. This regimen yielded a good response to therapy with a decrease in disease burden.
Case 5
A 28-year-old girl, operated for mucinous adenocarcinoma of the rectum, presented with recurrence at the anastomotic site, a year after the surgery. She also presented with a lump in the left breast, increasing in size over a period of 4 months. Mammography revealed high-density masses with partially obscured margins containing coarse calcifications in the upper outer quadrant of the left breast [Figure 5]A, [Figure 5]B. A targeted ultrasound revealed hypoechoic masses with irregular margins and calcifications within, showing posterior acoustic shadowing [Figure 5]C and [Figure 5]D. A core biopsy with IHC revealed features of metastases from mucinous adenocarcinoma, positive for CK20 and negative for CK7. The patient was then treated with palliative chemotherapy but was lost to follow-up.
Case 6
A 47-year-old lady presented with a history of nasal obstruction, worsening over a period of 6 months associated with mild proptosis of the right eye. A contrast-enhanced CT of the paranasal sinuses revealed an enhancing soft tissue in the right maxillary sinus and nasal cavity causing bony erosion with orbital extension [Figure 6]A. Histopathologic examination of the tissue revealed Non-Hodgkin's lymphoma (NHL) of the diffuse large B-cell type. She received six cycles of chemotherapy for the same. During the course of treatment, she developed painless lumps in bilateral breasts. Mammography revealed multiple well-circumscribed high-density masses involving all quadrants of bilateral breasts [Figure 6]B and [Figure 6]C. Ultrasonography revealed multiple hypoechoic masses with irregular margins showing posterior acoustic shadowing [Figure 6]D. A core biopsy with IHC revealed B-cell type of NHL, positive for CD20, consistent with metastases. The chemotherapy regimen was modified. However, the patient died of fungal pneumonia after 6 months.
The presence of a breast lesion in any patient with a known primary tumor elsewhere poses a diagnostic challenge to the clinician. The diagnostic approach first involves the differentiation of benign and malignant lesions, and if malignant, it is essential to know whether the lesion is primary or secondary since the treatment and prognosis differ greatly according to the nature of the lesion. Because of the rarity and unusual clinico-pathologic characteristics of breast metastases, it can be difficult to make an adequate diagnosis clinically and histologically.[1] This is particularly true if the breast abnormality is the first presentation of unknown extramammary primary cancers metastatic to the breast.[1],[2]
Metastases to the breast may occur years after the diagnosis of a primary cancer.[2] Clinical differentiation from a primary carcinoma is challenging as majority of metastases present as rapidly growing, painless, palpable, firm breast masses.[2] Radiology may play a critical role in aiding the diagnosis of metastatic breast disease. On mammography, metastases generally present as one or more well-circumscribed masses,[3] commonly located in the upper outer quadrants without spiculations, calcifications, and features of desmoplastic reaction that characterizes majority of primary carcinomas.[3],[4] Exceptions do occur, such as cases of mucinous adenocarcinomas of the rectum, as described in this article or metastatic ovarian carcinomas, in which metastatic lesions to the breast may reveal calcifications.[5]Diffuseparenchymal involvement mimicking inflammatory carcinoma can be seen rarely, which was seen in the case of metastatic stomach cancer that we encountered. A similar pattern has been described in a previously described case series, in which metastatic stomach cancer presented with diffuse parenchymal infiltration instead of a discrete mass.[3]
Ultrasonographic appearance of metastases may reveal solitary or multiple lesions, predominantly round or oval, with hypoechoic and solid echo patterns, with usually well-defined posterior margins. Multiple lesions are known to present with similar imaging findings.[3],[4] On ultrasound, hematogenous metastases tend to have circumscribed margins without spiculations, calcifications, architectural distortion, or posterior acoustic shadowing.[6] Lymphangitic metastases however manifest as diffuse skin and trabecular thickening because of obstruction of draining lymphatics.[6] On ultrasonography, metastases to the breast are usually seen in the subcutaneous tissue, as noted in most of our cases or immediately adjacent to the parenchyma.
The primary sources of breast metastases in our case series were leiomyosarcoma, gastric carcinoma, Ewing's sarcoma, cervical carcinoma, colorectal carcinoma, and NHL.
The mammographic features of metastatic leiomyosarcoma to the breast, in our case, were similar to the one reported by Vizcaino et al.[7] Both cases presented as discrete, well-circumscribed masses, though our patient had a single deposit and Vizcaino et al. reported multiple deposits.[7]Two other cases of metastases from a primary leiomyosarcoma have been reported in literature;[8],[9] however, the uterine origin of these deposits has not been documented.
Metastatic gastric adenocarcinoma to the breast has been reported to have variable imaging features. The case reported by Qureshi et al. did not present with suspicious imaging features and was diagnosed purely on histopathology.[10] In the case reported by Cavazzini et al., the clinical features were similar to the ones reported by us; however, the imaging features differed. They reported an irregular poorly defined mass without calcifications, whereas our patient presented with a diffuse increase in parenchymal density with thickening of the nipple–areola complex.[11]Kwak et al. reported two cases of metastatic signet ring cell carcinoma with increased parenchymal density on mammography mimicking inflammatory breast carcinoma, similar to our case; however, the organ of origin was not confirmed.[12]
Vergier et al. reported a case of metastasis to the breast in a patient of epidermoid cervical carcinoma; however, the metastatic deposit in their case was found to have spiculated margins.[13] Rarely, metastasis from cervical carcinoma may mimic an inflammatory breast cancer as reported by Ward et al.[14] The imaging features in our case differed from both of these as the deposit in our case was a discrete, well-circumscribed mass.
Mihai et al. reported a case of breast metastasis suspected to be from a primary rectal carcinoma with imaging features not characteristic for malignancy, appearing as a well-defined mass on mammography; however, the organ of origin could not be confirmed.[15] Li et al. and Zhang et al. reported cases of poorly differentiated adenocarcinoma of the rectum with metastasis to the breast presenting as an indistinctly marginated mass.[16],[17] Ahmad et al. reported metastases to the breast from well-differentiated colo-rectal adenocarcinoma presenting as a partially well-defined nodule with intermediate type of microcalcifications on mammography, which suggested suspicious morphology favoring primary breast carcinoma; however, it later turned out to be metastatic deposit from a colo-rectal primary.[18] Our case differed from the above cases as we encountered an extremely rare form of metastasis presenting with coarse calcifications, which differed from all of these.
Very few cases of metastases to the breast from Ewing' sarcoma have been documented. Örgüç et al. have reported a case of breast metastasis from Ewing's sarcoma of the right iliac bone in a 12-year-old girl, with imaging features similar to ours.[19]
NHL of the breast is an extremely rare occurrence, accounting for about 0.5% of all breast malignancies and 1% of NHL,[20],[21] and usually manifests as a secondary disease (i.e., in association with extramammary NHL).[21] Surov et al. studied the imaging features of breast lymphoma in 36 patients. The most common mammographic finding in their study was multiple intramammary masses with circumscribed or microlobulated margins, similar to our case.[21] The ultrasound features were also identical to ours, with most lesions appearing as hypoechoic, oval, or round masses with circumscribed margins. In the study by Yang et al., most cases of breast lymphoma however presented with a solitary breast mass with indistinct or irregular margins on mammography and ultrasound, which differed from the findings in our study.[22]
In conclusion, our case series provides an overview of unusual cases of metastases to the breast from various extramammary malignancies. The occurrence of a breast mass in a patient with a known primary must be approached with caution, and the possibility of metastasis must be excluded, as the disease prognosis and course of management can be ascertained only after this distinction is made.
The discovery of a breast mass in a patient with a known primary tumor elsewhere or with a previous history of cancer at another site poses a diagnostic challenge to the clinician. An awareness of the various malignancies that can metastasize to the breast and accurate diagnosis of the same is essential in order to avoid an unnecessary mastectomy and to guide further therapy.
In this article, we present six cases of metastases to the breast, in patients with a primary extramammary malignancy. Metastases in these primary tumors are exceedingly rare, and hence, this case series would serve as a valuable addition to the existing literature. In addition, we present a review on the subject with an emphasis on imaging findings.
Case 1
A 40-year-old lady presented with menorrhagia for about 8 months. She underwent a contrast-enhanced CT scan of the abdomen and pelvis, which revealed a heterogeneously enhancing myometrial mass, with atypical imaging features [Figure 1]A. There was no evidence of distant metastases on cross-sectional imaging. The patient underwent a total hysterectomy with a bilateral salpingo-oophorectomy. Histopathological evaluation of the myometrial mass revealed an intermediate grade leiomyosarcoma (Immunohistochemistry IHC – Mib labeling index of 50%). Thereafter, she presented with a lump in the right breast, progressively increasing in size over a period of 6 months.
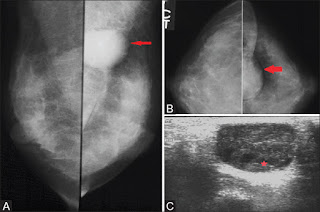
 | Figure 1 (A-D): (A) Coronal sections of contrast-enhanced CT pelvis images showing a heterogeneously enhancing mass involving the myometrium of the uterine fundus (red arrows). (C and D) Right mammogram (extended CC view (C) and MLO view (D)) showing a well-circumscribed isodense mass in the upper outer quadrant of the right breast (red asterisk). (B) Ultrasonography image showing a well-defined, round hypoechoic mass at the 10 o'clock position in the right breast Click here to view |
Mammography revealed the presence of a well-circumscribed isodense mass in the upper outer quadrant of the right breast [Figure 1]C and [Figure 1]D. Breast ultrasonography demonstrated a well-defined solid, hypoechoic mass with mild posterior acoustic enhancement, at the site of palpable abnormality [Figure 1]B. A core biopsy of the lesion revealed a spindle cell tumor exhibiting focally moderate to marked nuclear atypia. On IHC, tumor cells were positive for smooth muscle actin, desmin, H-caldesmon and showed a high Mib-1 count. The histopathology report was conclusive for leiomyosarcoma in the clinical context. A contrast-enhanced CT abdomen scan was subsequently done which revealed a metastatic lesion in the liver and a retroperitoneal metastatic nodal mass. Thereafter, the patient received palliative chemotherapy for 2 years but did not survive.
Case 2
A 31-year-old lady, with poorly differentiated adenocarcinoma of the stomach (stage T3N2M0), underwent a radical gastrectomy. She was receiving adjuvant chemo-radiotherapy (CT-RT) during which she developed abdominal distention, along with diffuse pain in the left breast with redness of the overlying skin over a period of 1 month. A contrast-enhanced CT scan of the thorax and abdomen with a mammogram was performed. Contrast-enhanced CT of the thorax and abdomen revealed ill-defined enhancement in the left breast [Figure 2]A.
 | Figure 2 (A-C): (A) Axial sections of contrast-enhanced CT thorax images showing diffuse ill-defined enhancement in the left breast (red arrows). (B) Bilateral mammograms (CC view) showing a diffuse increase in density in the left breast (red arrows), with thickening of the overlying skin and the nipple–areola complex (red asterisks). (C) Ultrasonography image showing an ill-defined hypoechoic lesion replacing the fibro-glandular parenchyma of the left breast (red asterisk) Click here to view |
Mammography revealed a diffuse increase in density involving the left breast, with thickening of the overlying skin and the nipple–areola complex [Figure 2]B. Breast ultrasonography demonstrated an ill-defined hypoechoic lesion replacing the fibro-glandular parenchyma [Figure 2]C. A left breast core biopsy revealed poorly differentiated carcinoma with signet ring cell morphology. Immunohistochemistry revealed positivity for CK 7, ER, CDX2, CK 20, and GCDFP, which was consistent with metastasis from carcinoma stomach. Contrast-enhanced CT abdomen revealed ascites with peritoneal metastases. The patient is being treated with palliative chemotherapy since then, with stable disease.
Case 3
A 37-year-old lady, with carcinoma cervix (stage IIIa) receiving concomitant chemoradiation and brachytherapy for the same, developed a lump in the left breast, gradually increasing over a period of 3 months. A mammogram and a screening ultrasonography of the abdomen were performed.
Mammography revealed a well-circumscribed, isodense mass in the upper central region of the left breast [Figure 3]A and [Figure 3]B. A breast ultrasound revealed a predominantly hypoechoic lesion in the upper central region showing mild internal vascularity [Figure 3]C. Fine-needle aspiration of the lesion revealed clusters of squamous epithelial cells, consistent with metastasis from cervical carcinoma. An ultrasound of the abdomen revealed evidence of liver metastases. The patient was put on palliative chemotherapy, is now being followed up annually.
 | Figure 3 (A-C): (A and B) Bilateral mammograms (MLO view (A) and CC view (B)) showing a well-circumscribed, isodense mass in the upper central region of the left breast (red arrows). (C) Ultrasonography image showing a well-defined hypoechoic lesion at the 12 o'clock position in the left breast (red asterisk) Click here to view |
Case 4
A 16-year-old girl, with Ewing's sarcoma of the left ninth rib being treated with chemotherapy, presented with a slow growing lump in the left breast. About 3 months after commencement of therapy, a contrast-enhanced CT of the thorax was performed for monitoring disease response. The CT revealed a heterogeneously enhancing mass involving the left ninth rib causing bony destruction with intrathoracic extension. In addition, an irregular heterogeneously enhancing mass with central necrosis was also seen incidentally in the left breast. Bilateral pleural effusion was seen [Figure 4]A,[Figure 4]B,[Figure 4]C. A breast ultrasound revealed a predominantly hypoechoic mass with irregular margins in the upper central region [Figure 4]D. A fine-needle aspiration cytology study of the left breast mass revealed cytologic features of PNET (Primitive neuro-ectodermal tumor)/Ewing's sarcoma with positivity for CD99, consistent with metastases from the primary. The patient was treated with systemic chemotherapy and received radiotherapy to the breast. This regimen yielded a good response to therapy with a decrease in disease burden.
 | Figure 4 (A-D): (A) Axial contrast-enhanced CT image of the thorax showing a heterogeneously enhancing mass with irregular margins in the left breast (yellow arrow). Incidentally seen is bilateral pleural effusion. (B) Sagittal contrast-enhanced CT image of the thorax showing a heterogeneously enhancing soft tissue with erosion of the left ninth rib (red arrow). A heterogeneously enhancing mass with irregular margins is seen in the left breast (yellow arrow). (C) Coronal bone window sections of the thorax showing permeative destruction of the left ninth rib (red arrow). (D) Ultrasonography image showing a heterogeneous mass with irregular margins in the left breast Click here to view |
Case 5
A 28-year-old girl, operated for mucinous adenocarcinoma of the rectum, presented with recurrence at the anastomotic site, a year after the surgery. She also presented with a lump in the left breast, increasing in size over a period of 4 months. Mammography revealed high-density masses with partially obscured margins containing coarse calcifications in the upper outer quadrant of the left breast [Figure 5]A, [Figure 5]B. A targeted ultrasound revealed hypoechoic masses with irregular margins and calcifications within, showing posterior acoustic shadowing [Figure 5]C and [Figure 5]D. A core biopsy with IHC revealed features of metastases from mucinous adenocarcinoma, positive for CK20 and negative for CK7. The patient was then treated with palliative chemotherapy but was lost to follow-up.
 | Figure 5 (A-D): (A and B) Left mammogram ((A) CC view and (B) MLO view) showing high-density masses (red arrows) with partially obscured margins containing coarse calcifications (yellow arrows and yellow asterisk) in the upper outer quadrant of the left breast. (C and D) Ultrasound images showing hypoechoic masses with irregular margins and coarse calcifications within, showing posterior acoustic shadowing (red arrow) at the 2 o'clock position in the left breast Click here to view |
Case 6
A 47-year-old lady presented with a history of nasal obstruction, worsening over a period of 6 months associated with mild proptosis of the right eye. A contrast-enhanced CT of the paranasal sinuses revealed an enhancing soft tissue in the right maxillary sinus and nasal cavity causing bony erosion with orbital extension [Figure 6]A. Histopathologic examination of the tissue revealed Non-Hodgkin's lymphoma (NHL) of the diffuse large B-cell type. She received six cycles of chemotherapy for the same. During the course of treatment, she developed painless lumps in bilateral breasts. Mammography revealed multiple well-circumscribed high-density masses involving all quadrants of bilateral breasts [Figure 6]B and [Figure 6]C. Ultrasonography revealed multiple hypoechoic masses with irregular margins showing posterior acoustic shadowing [Figure 6]D. A core biopsy with IHC revealed B-cell type of NHL, positive for CD20, consistent with metastases. The chemotherapy regimen was modified. However, the patient died of fungal pneumonia after 6 months.
 | Figure 6 (A-D): (A) Contrast-enhanced coronal CT image of the paranasal sinuses showing an enhancing soft tissue (red asterisk) in the right maxillary sinus extending to the ethmoidal sinuses and nasal cavity causing bony erosion with orbital extension. (B and C) Bilateral mammograms ((B) MLO view and (C) CC view) showing multiple well-circumscribed high-density masses involving all quadrants of bilateral breasts (red asterisks). (D) Ultrasonography images showing darkly hypoechoic masses with indistinct margins (yellow asterisks) Click here to view |
 Discussion Discussion |  |
The presence of a breast lesion in any patient with a known primary tumor elsewhere poses a diagnostic challenge to the clinician. The diagnostic approach first involves the differentiation of benign and malignant lesions, and if malignant, it is essential to know whether the lesion is primary or secondary since the treatment and prognosis differ greatly according to the nature of the lesion. Because of the rarity and unusual clinico-pathologic characteristics of breast metastases, it can be difficult to make an adequate diagnosis clinically and histologically.[1] This is particularly true if the breast abnormality is the first presentation of unknown extramammary primary cancers metastatic to the breast.[1],[2]
Metastases to the breast may occur years after the diagnosis of a primary cancer.[2] Clinical differentiation from a primary carcinoma is challenging as majority of metastases present as rapidly growing, painless, palpable, firm breast masses.[2] Radiology may play a critical role in aiding the diagnosis of metastatic breast disease. On mammography, metastases generally present as one or more well-circumscribed masses,[3] commonly located in the upper outer quadrants without spiculations, calcifications, and features of desmoplastic reaction that characterizes majority of primary carcinomas.[3],[4] Exceptions do occur, such as cases of mucinous adenocarcinomas of the rectum, as described in this article or metastatic ovarian carcinomas, in which metastatic lesions to the breast may reveal calcifications.[5]Diffuseparenchymal involvement mimicking inflammatory carcinoma can be seen rarely, which was seen in the case of metastatic stomach cancer that we encountered. A similar pattern has been described in a previously described case series, in which metastatic stomach cancer presented with diffuse parenchymal infiltration instead of a discrete mass.[3]
Ultrasonographic appearance of metastases may reveal solitary or multiple lesions, predominantly round or oval, with hypoechoic and solid echo patterns, with usually well-defined posterior margins. Multiple lesions are known to present with similar imaging findings.[3],[4] On ultrasound, hematogenous metastases tend to have circumscribed margins without spiculations, calcifications, architectural distortion, or posterior acoustic shadowing.[6] Lymphangitic metastases however manifest as diffuse skin and trabecular thickening because of obstruction of draining lymphatics.[6] On ultrasonography, metastases to the breast are usually seen in the subcutaneous tissue, as noted in most of our cases or immediately adjacent to the parenchyma.
The primary sources of breast metastases in our case series were leiomyosarcoma, gastric carcinoma, Ewing's sarcoma, cervical carcinoma, colorectal carcinoma, and NHL.
The mammographic features of metastatic leiomyosarcoma to the breast, in our case, were similar to the one reported by Vizcaino et al.[7] Both cases presented as discrete, well-circumscribed masses, though our patient had a single deposit and Vizcaino et al. reported multiple deposits.[7]Two other cases of metastases from a primary leiomyosarcoma have been reported in literature;[8],[9] however, the uterine origin of these deposits has not been documented.
Metastatic gastric adenocarcinoma to the breast has been reported to have variable imaging features. The case reported by Qureshi et al. did not present with suspicious imaging features and was diagnosed purely on histopathology.[10] In the case reported by Cavazzini et al., the clinical features were similar to the ones reported by us; however, the imaging features differed. They reported an irregular poorly defined mass without calcifications, whereas our patient presented with a diffuse increase in parenchymal density with thickening of the nipple–areola complex.[11]Kwak et al. reported two cases of metastatic signet ring cell carcinoma with increased parenchymal density on mammography mimicking inflammatory breast carcinoma, similar to our case; however, the organ of origin was not confirmed.[12]
Vergier et al. reported a case of metastasis to the breast in a patient of epidermoid cervical carcinoma; however, the metastatic deposit in their case was found to have spiculated margins.[13] Rarely, metastasis from cervical carcinoma may mimic an inflammatory breast cancer as reported by Ward et al.[14] The imaging features in our case differed from both of these as the deposit in our case was a discrete, well-circumscribed mass.
Mihai et al. reported a case of breast metastasis suspected to be from a primary rectal carcinoma with imaging features not characteristic for malignancy, appearing as a well-defined mass on mammography; however, the organ of origin could not be confirmed.[15] Li et al. and Zhang et al. reported cases of poorly differentiated adenocarcinoma of the rectum with metastasis to the breast presenting as an indistinctly marginated mass.[16],[17] Ahmad et al. reported metastases to the breast from well-differentiated colo-rectal adenocarcinoma presenting as a partially well-defined nodule with intermediate type of microcalcifications on mammography, which suggested suspicious morphology favoring primary breast carcinoma; however, it later turned out to be metastatic deposit from a colo-rectal primary.[18] Our case differed from the above cases as we encountered an extremely rare form of metastasis presenting with coarse calcifications, which differed from all of these.
Very few cases of metastases to the breast from Ewing' sarcoma have been documented. Örgüç et al. have reported a case of breast metastasis from Ewing's sarcoma of the right iliac bone in a 12-year-old girl, with imaging features similar to ours.[19]
NHL of the breast is an extremely rare occurrence, accounting for about 0.5% of all breast malignancies and 1% of NHL,[20],[21] and usually manifests as a secondary disease (i.e., in association with extramammary NHL).[21] Surov et al. studied the imaging features of breast lymphoma in 36 patients. The most common mammographic finding in their study was multiple intramammary masses with circumscribed or microlobulated margins, similar to our case.[21] The ultrasound features were also identical to ours, with most lesions appearing as hypoechoic, oval, or round masses with circumscribed margins. In the study by Yang et al., most cases of breast lymphoma however presented with a solitary breast mass with indistinct or irregular margins on mammography and ultrasound, which differed from the findings in our study.[22]
In conclusion, our case series provides an overview of unusual cases of metastases to the breast from various extramammary malignancies. The occurrence of a breast mass in a patient with a known primary must be approached with caution, and the possibility of metastasis must be excluded, as the disease prognosis and course of management can be ascertained only after this distinction is made.








Δεν υπάρχουν σχόλια:
Δημοσίευση σχολίου
Medicine by Alexandros G. Sfakianakis,Anapafseos 5 Agios Nikolaos 72100 Crete Greece,00302841026182,00306932607174,alsfakia@gmail.com,